Guideline for Venous Thromboembolism Prophylaxis
Authors: Nicholas Carter, MD, Merce Miranda APRN, Brandon Parker DO – 108/24
Approval: Namias, Lineen, Jagid, Levi, Gebhard, Vilella – 10/8/24
Purpose
Ryder Trauma Division guidance for management of venous thromboembolism (VTE) mechanical and chemical prophylaxis including agent, timing of initiation, and indications for holding prophylaxis.
Mechanical prophylaxis
Sequential compression devices are recommended for all trauma patients while in bed except those with lower extremity injuries precluding safe positioning.
Chemical prophylaxis
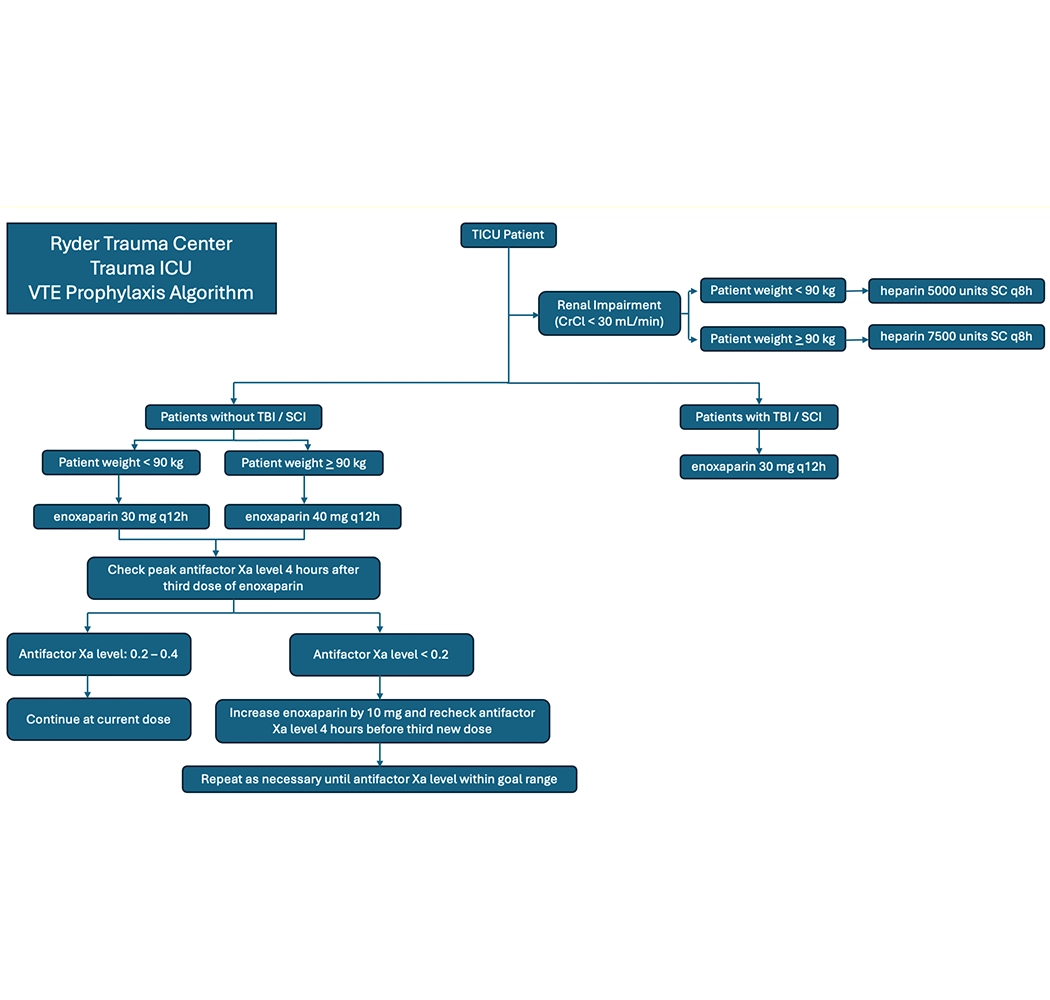
Trauma Patients:
Weight < 95 kg: enoxaparin 30 mg subcutaneously every 12 hours.
Weight > 95 kg: enoxaparin 40 mg subcutaneously every 12 hours.
After starting enoxaparin, check peak anti-Xa level 4 hours after the third dose.
If anti-Xa is 0.2 to 0.4, continue the current dose.
If anti-Xa is below 0.2, increase enoxaparin by 10 mg and recheck after the third new dose.
Repeat adjustments until the anti-Xa level is in range
If renal impairment with CrCl < 30 mL/min:
Weight < 95 kg: heparin 5,000 units subcutaneously every 8 hours.
Weight > 95 kg: heparin 7,500 units subcutaneously every 8 hours.
Patients with TBI/SCI:
Enoxaparin 30 mg subcutaneously every 12 hours.
Purpose
Ryder Trauma Division guidance for management of venous thromboembolism (VTE) mechanical and chemical prophylaxis including agent, timing of initiation, and indications for holding prophylaxis.
Mechanical prophylaxis
Sequential compression devices are recommended for all trauma patients while in bed except those with lower extremity injuries precluding safe positioning.
Chemical prophylaxis
Trauma Patients:
Weight < 95 kg: enoxaparin 30 mg subcutaneously every 12 hours.
Weight > 95 kg: enoxaparin 40 mg subcutaneously every 12 hours.
After starting enoxaparin, check peak anti-Xa level 4 hours after the third dose.
If anti-Xa is 0.2 to 0.4, continue the current dose.
If anti-Xa is below 0.2, increase enoxaparin by 10 mg and recheck after the third new dose.
Repeat adjustments until the anti-Xa level is in range
If renal impairment with CrCl < 30 mL/min:
Weight < 95 kg: heparin 5,000 units subcutaneously every 8 hours.
Weight > 95 kg: heparin 7,500 units subcutaneously every 8 hours.
Patients with TBI/SCI:
Enoxaparin 30 mg subcutaneously every 12 hours.
Monitoring on enoxaparin for ICU patients
- Check an anti-factor Xa level 4 hours after the third dose of enoxaparin.
- Goal anti-factor Xa level for prophylaxis is 0.2 – 0.4.
- If low, recommend increase of enoxaparin dose by 10mg and recheck after the third new dose.
NOT FOR TBI, SCI, IMCU, OR FLOOR PATIENTS.
- Patients transferred out of the TICU should remain on their adjusted dose.
Monitoring on enoxaparin for ICU patients
- Check an anti-factor Xa level 4 hours after the third dose of enoxaparin.
- Goal anti-factor Xa level for prophylaxis is 0.2 – 0.4.
- If low, recommend increase of enoxaparin dose by 10mg and recheck after the third new dose.
NOT FOR TBI, SCI, IMCU, OR FLOOR PATIENTS.
- Patients transferred out of the TICU should remain on their adjusted dose.
Indications for holding chemical prophylaxis
- Active bleeding (discretion of trauma surgery and/or ICU attending)
- Intracranial or spinal operations (see below)
- Insertion, manipulation, or removal of epidural catheter (see below)
Indications for holding chemical prophylaxis
- Active bleeding (discretion of trauma surgery and/or ICU attending)
- Intracranial or spinal operations (see below)
- Insertion, manipulation, or removal of epidural catheter (see below)
Process for varying practice from those outlined here as agreed upon by invested parties and supported by evidence:
- The attending of the service requesting variation should speak with the TICU attending
- If an agreement on appropriate therapy cannot be reached, then Unit Director or Dr. Namias will be contacted for further discussion
Process for varying practice from those outlined here as agreed upon by invested parties and supported by evidence:
- The attending of the service requesting variation should speak with the TICU attending
- If an agreement on appropriate therapy cannot be reached, then Unit Director or Dr. Namias will be contacted for further discussion
Screening and Surveillance of high-risk patients
SEE SEPARATE GUIDLINE FOR VTE SCREENING FOR DETAILED DESCRIPTION
Risk assessment profile (RAP) score calculated for all patients at admission by admitting fellow or Nurse Practitioner during rounds.
For patients with RAP score > or equal to 8, admission and weekly (while in ICU) lower extremity venous duplex ultrasound and 24 hr Creatinine Clearance.
Screening and Surveillance of high-risk patients
SEE SEPARATE GUIDLINE FOR VTE SCREENING FOR DETAILED DESCRIPTION
Risk assessment profile (RAP) score calculated for all patients at admission by admitting fellow or Nurse Practitioner during rounds.
For patients with RAP score > or equal to 8, admission and weekly (while in ICU) lower extremity venous duplex ultrasound and 24 hr Creatinine Clearance.
Special Circumstances
VTE Chemoprophylaxis in Solid Organ Injury:
Chemoprophylaxis at above recommended dosing should begin within 24-48 hours if no signs of ongoing bleeding and no other contraindications. (Hemoglobin must be stable)
VTE Chemoprophylaxis following angioembolization:
Chemoprophylaxis at above recommended dosing should be within 24-48 hours following procedure if no signs of ongoing bleeding and no other contraindications. (Hemoglobin must be stable)
VTE Chemoprophylaxis and Neuraxial Anesthesia:
Patients with an epidural catheter in place should receive chemical prophylaxis with subcutaneous heparin 5000U 3x/day unless otherwise contraindicated. With the exception of aspirin, all antiplatelet and anticoagulant agents should be held before and after insertion, manipulation, and removal of epidural catheters. The table below describes the recommended duration for holding common agents.
Special Circumstances
VTE Chemoprophylaxis in Solid Organ Injury:
Chemoprophylaxis at above recommended dosing should begin within 24-48 hours if no signs of ongoing bleeding and no other contraindications. (Hemoglobin must be stable)
VTE Chemoprophylaxis following angioembolization:
Chemoprophylaxis at above recommended dosing should be within 24-48 hours following procedure if no signs of ongoing bleeding and no other contraindications. (Hemoglobin must be stable)
VTE Chemoprophylaxis and Neuraxial Anesthesia:
Patients with an epidural catheter in place should receive chemical prophylaxis with subcutaneous heparin 5000U 3x/day unless otherwise contraindicated. With the exception of aspirin, all antiplatelet and anticoagulant agents should be held before and after insertion, manipulation, and removal of epidural catheters. The table below describes the recommended duration for holding common agents.
Agent Specific timing for Neuraxial Anesthesia:
Description
Agent Specific timing for Neuraxial Anesthesia:
Subcutaneous Heparin
- Time held prior to insertion and removal: 4–6 hours
- Time held following insertion, manipulation, and removal: 1 hour
Single Daily Prophylactic-dose Enoxaparin
- Time held prior to insertion and removal: 12 hours
- Restart after insertion: 12 hours
- Restart after removal: 4 hours
Twice Daily Prophylactic-dose Enoxaparin
- Time held prior to insertion and removal: 24 hours (cannot be continued if epidural catheter is in place)
- While catheter is in place: Switch to single daily dosing
- Restart twice daily dosing: 4 hours after catheter removal
Therapeutic-dose Enoxaparin
- Time held prior to insertion and removal: 24 hours (cannot be continued while epidural catheter is in place)
- While catheter is in place: Switch to single daily dosing
- Restart therapeutic dosing: 4 hours after catheter removal
Heparin Infusion
- Time held prior to insertion and removal: 4–6 hours with verified normal coagulation status
- Time held following insertion, manipulation, and removal: 1 hour
Argatroban Infusion
- Time held prior to insertion and removal: Unknown / no recommendation
- Restarting after catheter placement: Cannot be restarted with epidural catheter in place
Aspirin
- Time held prior to insertion and removal: Unnecessary to hold
- Time held following insertion, manipulation, and removal: Unnecessary to hold
Clopidogrel
- Time held prior to insertion and removal: 7 days
- Restart following removal: Immediately, unless loading dose is administered
Subcutaneous Heparin
- Time held prior to insertion and removal: 4–6 hours
- Time held following insertion, manipulation, and removal: 1 hour
Single Daily Prophylactic-dose Enoxaparin
- Time held prior to insertion and removal: 12 hours
- Restart after insertion: 12 hours
- Restart after removal: 4 hours
Twice Daily Prophylactic-dose Enoxaparin
- Time held prior to insertion and removal: 24 hours (cannot be continued if epidural catheter is in place)
- While catheter is in place: Switch to single daily dosing
- Restart twice daily dosing: 4 hours after catheter removal
Therapeutic-dose Enoxaparin
- Time held prior to insertion and removal: 24 hours (cannot be continued while epidural catheter is in place)
- While catheter is in place: Switch to single daily dosing
- Restart therapeutic dosing: 4 hours after catheter removal
Heparin Infusion
- Time held prior to insertion and removal: 4–6 hours with verified normal coagulation status
- Time held following insertion, manipulation, and removal: 1 hour
Argatroban Infusion
- Time held prior to insertion and removal: Unknown / no recommendation
- Restarting after catheter placement: Cannot be restarted with epidural catheter in place
Aspirin
- Time held prior to insertion and removal: Unnecessary to hold
- Time held following insertion, manipulation, and removal: Unnecessary to hold
Clopidogrel
- Time held prior to insertion and removal: 7 days
- Restart following removal: Immediately, unless loading dose is administered
Traumatic Brain Injury
Patients with traumatic brain injury should generally receive Enoxaparin 30mg 2x/day 24 hours post stable head CT.
Traumatic Brain Injury
Patients with traumatic brain injury should generally receive Enoxaparin 30mg 2x/day 24 hours post stable head CT.
Spinal Trauma
Patients with spinal cord injuries should generally receive enoxaparin 30mg 2x/day at 48 hours post-injury. Patients who undergo spine operations should have chemical prophylaxis held the morning of their operation and resumed not sooner than 24 hours after their operation.
Follow TBI guidelines for patients with spinal injury and concomitant TBI.
Spinal Trauma
Patients with spinal cord injuries should generally receive enoxaparin 30mg 2x/day at 48 hours post-injury. Patients who undergo spine operations should have chemical prophylaxis held the morning of their operation and resumed not sooner than 24 hours after their operation.
Follow TBI guidelines for patients with spinal injury and concomitant TBI.
Orthopedic Surgery
Preoperative chemical VTE prophylaxis does not need to be held for orthopedic procedures unless requested by the attending orthopedic surgeon due to case specific factors or in the following procedure:
- Fixation of acetabular fracture
Orthopedic Surgery
Preoperative chemical VTE prophylaxis does not need to be held for orthopedic procedures unless requested by the attending orthopedic surgeon due to case specific factors or in the following procedure:
- Fixation of acetabular fracture
Acute Care Surgery
Preoperative chemical VTE prophylaxis does not need to be held unless requested by the attending surgeon.
Acute Care Surgery
Preoperative chemical VTE prophylaxis does not need to be held unless requested by the attending surgeon.
References
Ley et al. Updated Guidelines to Reduce Venous Thromboembolism in Trauma Patients: A Western Trauma Association Critical Decisions Algorithm. (Journal of Trauma and Acute Care Surgery 2020; 89:5, 971-981).
Vandermeuelen et al. Regional Anesthesia in the Patient Receiving Antithrombotic or Thrombolytic Therapy American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guidelines (Fourth Edition) (Reg Anesth Pain Med 2018;43: 263–309).
Guidelines for the Management of Severe Traumatic Brain Injury (Fourth Edition). American Association of Neurological Surgeons and the Congress of Neurological Surgeons. Sept 2016.
Barrera LM, Perel P, Ker K, Cirocchi R, Farinella E, Morales Uribe CH: Thromboprophylaxis for trauma patients. Cochrane Database Syst Rev 2013;3:CD008303.
Scolaro et al. Venous Thromboembolism in Orthopaedic Trauma. (Journal of the American Academy of Orthopaedic Surgeons: January 2015 – Volume 23 – Issue 1 – p 1-6)
References
Ley et al. Updated Guidelines to Reduce Venous Thromboembolism in Trauma Patients: A Western Trauma Association Critical Decisions Algorithm. (Journal of Trauma and Acute Care Surgery 2020; 89:5, 971-981).
Vandermeuelen et al. Regional Anesthesia in the Patient Receiving Antithrombotic or Thrombolytic Therapy American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guidelines (Fourth Edition) (Reg Anesth Pain Med 2018;43: 263–309).
Guidelines for the Management of Severe Traumatic Brain Injury (Fourth Edition). American Association of Neurological Surgeons and the Congress of Neurological Surgeons. Sept 2016.
Barrera LM, Perel P, Ker K, Cirocchi R, Farinella E, Morales Uribe CH: Thromboprophylaxis for trauma patients. Cochrane Database Syst Rev 2013;3:CD008303.
Scolaro et al. Venous Thromboembolism in Orthopaedic Trauma. (Journal of the American Academy of Orthopaedic Surgeons: January 2015 – Volume 23 – Issue 1 – p 1-6)