ICU Sedation and Analgesia
Authors: Jennifer Lobb, Roman Dudaryk, Gina Riggi, Brandon Parker – 4/06/22
Approval: : Lineen, Namias – 6/6/22
Goals
- To improve patient outcomes by reducing the number of days that patients are on mechanical ventilation and in the ICU.
- To improve pain control in the ICU in acute and subacute setting.
- To clearly delineate roles in the process of improving pain and sedation amongst prescribers (physicians and nurse practitioners), pharmacists, bedside nurses and nurse managers
- Providers: To encourage responsible opiate prescribing to improve patient outcomes and to encourage use of multiple modalities of pain management (opioid sparing)
- Nurses and providers: To relieve pain without altering sensorium whenever possible
- Nurses and providers: To prevent and treat delirium in the ICU
- Nurse managers: To ensure compliance with prescribed medications and care parameters (lights on, head of bed elevated, physical restraints, etc.)
- Pharmacists: To assess adherence to protocols and provide guidance and insight when necessary
General Guidelines
- Pain often leads to agitation. The primary goal in the TICU should be pain and discomfort control, and then, if necessary, sedation should be performed.
- PRN medications should be used preferentially over infusions
- A routine assessment of the patient should be done by both nurses (q4h) and prescribers (q4h, PRN) to determine whether any issues are pain or sedation related:
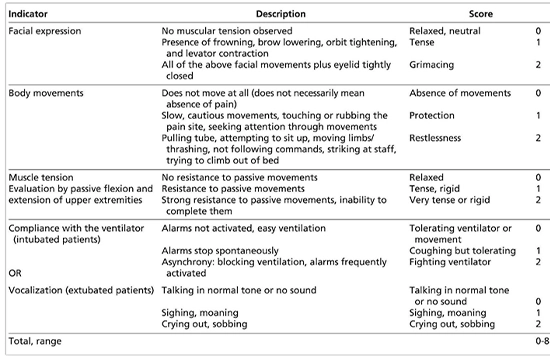
- Signs of pain: Grimacing, pulling at lines/tubes, resistance to passive motion, ventilator alarming, sighing or crying (in non-ventilated patients). See Critical Care Pain Observation Tool (CPOT) table below
- Target goals for pain and sedation: (UNLESS OTHERWISE STATED)
- CPOT score of 0-2
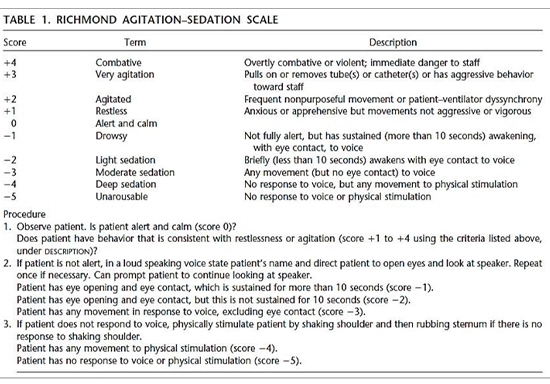
- RASS of 0 to -2
- Nurses: Use of PRN medications before increasing dose on infusion rate, as infusions take approximately 1 hour to take effect, while PRN administrations act immediately
- Infusion medications also increase risk of over-medicating which can lead to longer length of stay, more time on the ventilator and potentially more ventilator associated pneumonia, delirium and death.
- Prescribers:
- A patient should never be placed on a sedation infusion without first assessing pain and providing appropriate pain control (via PRN or infusion)
- Focus on multimodal pain management: multiple medications in therapeutic range as opposed to few medications at high/toxic range
- Pharmacists: Daily rounding with ICU team to provide suggestions and guidance on improving pain and sedation
Pain Assessment: Critical Care Pain Observation Tool (CPOT)
Goals
- To improve patient outcomes by reducing the number of days that patients are on mechanical ventilation and in the ICU.
- To improve pain control in the ICU in acute and subacute setting.
- To clearly delineate roles in the process of improving pain and sedation amongst prescribers (physicians and nurse practitioners), pharmacists, bedside nurses and nurse managers
- Providers: To encourage responsible opiate prescribing to improve patient outcomes and to encourage use of multiple modalities of pain management (opioid sparing)
- Nurses and providers: To relieve pain without altering sensorium whenever possible
- Nurses and providers: To prevent and treat delirium in the ICU
- Nurse managers: To ensure compliance with prescribed medications and care parameters (lights on, head of bed elevated, physical restraints, etc.)
- Pharmacists: To assess adherence to protocols and provide guidance and insight when necessary
General Guidelines
- Pain often leads to agitation. The primary goal in the TICU should be pain and discomfort control, and then, if necessary, sedation should be performed.
- PRN medications should be used preferentially over infusions
- A routine assessment of the patient should be done by both nurses (q4h) and prescribers (q4h, PRN) to determine whether any issues are pain or sedation related:
- Signs of pain: Grimacing, pulling at lines/tubes, resistance to passive motion, ventilator alarming, sighing or crying (in non-ventilated patients). See Critical Care Pain Observation Tool (CPOT) table below
- Target goals for pain and sedation: (UNLESS OTHERWISE STATED)
- CPOT score of 0-2
- RASS of 0 to -2
- Nurses: Use of PRN medications before increasing dose on infusion rate, as infusions take approximately 1 hour to take effect, while PRN administrations act immediately
- Infusion medications also increase risk of over-medicating which can lead to longer length of stay, more time on the ventilator and potentially more ventilator associated pneumonia, delirium and death.
- Prescribers:
- A patient should never be placed on a sedation infusion without first assessing pain and providing appropriate pain control (via PRN or infusion)
- Focus on multimodal pain management: multiple medications in therapeutic range as opposed to few medications at high/toxic range
- Pharmacists: Daily rounding with ICU team to provide suggestions and guidance on improving pain and sedation
Pain Assessment: Critical Care Pain Observation Tool (CPOT)
Sedation Assessment: Richmond Agitation-Sedation Scale (RASS)
Description
Sedation Assessment: Richmond Agitation-Sedation Scale (RASS)
Special Populations
- Geriatric patients (>65 years of age)
- Post-operative patients
- “Difficult patient” pathway
Geriatric Patients (>65 years of age)
- Medications
- First line on admission is IV acetaminophen
- Narcotic dosing should start at morphine 2mg
- Encourage multimodal and opiate sparing
- Melatonin QHS to aid with sleeping
- Focus on prevention and treatment of delirium while providing appropriate analgesia and sedation
- Daily sedation vacations and spontaneous breathing trials are MANDATORY!
- Do not prescribe benzodiazepines to elderly patients (if home med, may need to be tapered)
- Avoid diphenhydramine and other anticholinergics when possible.
- Aggressive weaning of opioids, as high doses of opioids have been shown to increase delirium
- Consider alternative non-opioid medications such as Tylenol, Tramadol,
- All patients should have lights on during sunlight hours and be up in a chair (when possible) during the day to normalize sleep/wake cycle.
Post-operative Patients
- Pain/sedation orders should be reviewed by the provider immediately upon return from OR to ICU and adjustments made as necessary. Examples:
- A patient who had a tracheostomy in the OR will should have discontinuation of sedation drips upon return to ICU
- A patient who underwent a re exploration of the abdomen may have an increase in pain after the OR
“Difficult Patient” Pathway
- Restart home psychiatric medication
- Consider standing quetiapine or ariprazole
- Utilize PRN
- Olanzapine
- Haloperidol
- Ziprasidone
Analgesia and Sedation Key Points
- Maintaining light levels of sedation in adult ICU patients is associated with IMPROVED clinical outcomes
- Shorter length of stay in the ICU
- Shorter duration of mechanical ventilation
- Evidence from randomized, controlled trials consistently supports the use of the minimum possible sedation
- Goal is light sedation (awake and cooperative, RASS Goal 0 to -2)
- Want the least amount of medication to achieve the desired effect
- If a patient is within the goal RASS and CPOT, then the doses should be titrated DOWN to minimize the risk of adverse events and tolerance from these medications
- A minority of patients have an indication for deep continuous sedation:
- Increased ICP
- Severe respiratory failure (example: acute respiratory distress syndrome)
- Refractory status epilepticus
- Prevention of awareness for patients receiving neuromuscular blockers
- It is important that prescribers use the Mechanical Ventilation Power Plan to order continuous and breakthrough analgesia and sedation orders. The Power Plan orders for the continuous medications have titration parameters and it prompts the prescriber to order breakthrough analgesia and sedation orders
- Fentanyl also has sedative properties, BOTH CPOT and RASS scores should be documented on patients that have continuous infusion fentanyl orders
- The equivalent dose of IV opioids is 1.5mg hydromorphone ~ 10mg IV morphine ~100 mcg fentanyl
Sedation and Analgesia FAQs
- Why should I titrate down the continuous analgesia/sedation if my patient is within the CPOT and RASS goal?
- When you have a patient that is on pressors and their MAP is within goal what do you do?
- We try to decrease the dose of the pressors to see if the patient maintains their MAP goal, it is the same concept with titrating down the sedation when the patient is with the CPOT and RASS goals
- When we do not titrate analgesia and sedation levels daily, we put the patient at risk for becoming TOLERANT to these medications.
- Risk factors for opioid and benzodiazepine withdrawal include the dose and duration (associated with one week or more of high dose therapy)
- When you have a patient that is on pressors and their MAP is within goal what do you do?
- What should I do if my patient becomes agitated?
- Remove agitating agent if possible (uncomfortable position and requesting to sit up, unnecessary drain or tube present, requesting corrective eye wear)
- Always try to give a PRN agent prior to increasing the rate of the continuous infusion. If there is not one available, ask the prescriber to add one!
- PRN breakthrough analgesia/sedation orders are available to order through the Mechanical Ventilation Power Plan
- It is difficult to assess PRN mild, moderate and severe levels of pain while a patient is receiving continuous infusion analgesia and sedation, the mechanical ventilation Power Plan orders are for ‘breakthrough’ analgesia or sedation
- If the patient still requires more analgesia/sedation, then increase the rate of the infusion
- My patient did not tolerate a sedation vacation yesterday, I do not want to cause harm to my patient, why should I try to perform a sedation vacation again today?
- KEEP TRYING EACH DAY ON EVERYONE
- Analgesia and sedation needs in the ICU are dynamic, just as vital signs and ventilator settings are dynamic
- If it is unsafe for all of the analgesia and sedation to be held for a sedation vacation, discuss with the ICU team the possibility of lowering the rate of the infusion or holding only the continuous infusion sedative (For example, continue the fentanyl infusion and hold the propofol infusion)
- A failed sedation vacation should indicate that we have successfully minimized our sedation
- If analgesia and sedation is assessed and titrated several times per day, then the sedation vacation will be easy to perform and is less likely to result in patient harm
BIS Score- GOAL 40-60
Paralytic titrated to train of four and sedation/analgesic titrated to BIS
- BIS 100: Awake
- BIS 80: Light moderated sedation
- BIS 60: General anesthesia
- BIS 40: Deep hypnotic sleep
- BIS 20: Comatose
- BIS 0: No brain activity
Description
Special Populations
- Geriatric patients (>65 years of age)
- Post-operative patients
- “Difficult patient” pathway
Geriatric Patients (>65 years of age)
- Medications
- First line on admission is IV acetaminophen
- Narcotic dosing should start at morphine 2mg
- Encourage multimodal and opiate sparing
- Melatonin QHS to aid with sleeping
- Focus on prevention and treatment of delirium while providing appropriate analgesia and sedation
- Daily sedation vacations and spontaneous breathing trials are MANDATORY!
- Do not prescribe benzodiazepines to elderly patients (if home med, may need to be tapered)
- Avoid diphenhydramine and other anticholinergics when possible.
- Aggressive weaning of opioids, as high doses of opioids have been shown to increase delirium
- Consider alternative non-opioid medications such as Tylenol, Tramadol,
- All patients should have lights on during sunlight hours and be up in a chair (when possible) during the day to normalize sleep/wake cycle.
Post-operative Patients
- Pain/sedation orders should be reviewed by the provider immediately upon return from OR to ICU and adjustments made as necessary. Examples:
- A patient who had a tracheostomy in the OR will should have discontinuation of sedation drips upon return to ICU
- A patient who underwent a re exploration of the abdomen may have an increase in pain after the OR
“Difficult Patient” Pathway
- Restart home psychiatric medication
- Consider standing quetiapine or ariprazole
- Utilize PRN
- Olanzapine
- Haloperidol
- Ziprasidone
Analgesia and Sedation Key Points
- Maintaining light levels of sedation in adult ICU patients is associated with IMPROVED clinical outcomes
- Shorter length of stay in the ICU
- Shorter duration of mechanical ventilation
- Evidence from randomized, controlled trials consistently supports the use of the minimum possible sedation
- Goal is light sedation (awake and cooperative, RASS Goal 0 to -2)
- Want the least amount of medication to achieve the desired effect
- If a patient is within the goal RASS and CPOT, then the doses should be titrated DOWN to minimize the risk of adverse events and tolerance from these medications
- A minority of patients have an indication for deep continuous sedation:
- Increased ICP
- Severe respiratory failure (example: acute respiratory distress syndrome)
- Refractory status epilepticus
- Prevention of awareness for patients receiving neuromuscular blockers
- It is important that prescribers use the Mechanical Ventilation Power Plan to order continuous and breakthrough analgesia and sedation orders. The Power Plan orders for the continuous medications have titration parameters and it prompts the prescriber to order breakthrough analgesia and sedation orders
- Fentanyl also has sedative properties, BOTH CPOT and RASS scores should be documented on patients that have continuous infusion fentanyl orders
- The equivalent dose of IV opioids is 1.5mg hydromorphone ~ 10mg IV morphine ~100 mcg fentanyl
Sedation and Analgesia FAQs
- Why should I titrate down the continuous analgesia/sedation if my patient is within the CPOT and RASS goal?
- When you have a patient that is on pressors and their MAP is within goal what do you do?
- We try to decrease the dose of the pressors to see if the patient maintains their MAP goal, it is the same concept with titrating down the sedation when the patient is with the CPOT and RASS goals
- When we do not titrate analgesia and sedation levels daily, we put the patient at risk for becoming TOLERANT to these medications.
- Risk factors for opioid and benzodiazepine withdrawal include the dose and duration (associated with one week or more of high dose therapy)
- When you have a patient that is on pressors and their MAP is within goal what do you do?
- What should I do if my patient becomes agitated?
- Remove agitating agent if possible (uncomfortable position and requesting to sit up, unnecessary drain or tube present, requesting corrective eye wear)
- Always try to give a PRN agent prior to increasing the rate of the continuous infusion. If there is not one available, ask the prescriber to add one!
- PRN breakthrough analgesia/sedation orders are available to order through the Mechanical Ventilation Power Plan
- It is difficult to assess PRN mild, moderate and severe levels of pain while a patient is receiving continuous infusion analgesia and sedation, the mechanical ventilation Power Plan orders are for ‘breakthrough’ analgesia or sedation
- If the patient still requires more analgesia/sedation, then increase the rate of the infusion
- My patient did not tolerate a sedation vacation yesterday, I do not want to cause harm to my patient, why should I try to perform a sedation vacation again today?
- KEEP TRYING EACH DAY ON EVERYONE
- Analgesia and sedation needs in the ICU are dynamic, just as vital signs and ventilator settings are dynamic
- If it is unsafe for all of the analgesia and sedation to be held for a sedation vacation, discuss with the ICU team the possibility of lowering the rate of the infusion or holding only the continuous infusion sedative (For example, continue the fentanyl infusion and hold the propofol infusion)
- A failed sedation vacation should indicate that we have successfully minimized our sedation
- If analgesia and sedation is assessed and titrated several times per day, then the sedation vacation will be easy to perform and is less likely to result in patient harm
BIS Score- GOAL 40-60
Paralytic titrated to train of four and sedation/analgesic titrated to BIS
- BIS 100: Awake
- BIS 80: Light moderated sedation
- BIS 60: General anesthesia
- BIS 40: Deep hypnotic sleep
- BIS 20: Comatose
- BIS 0: No brain activity