Direct Admissions to Orthopaedic Trauma Service
Authors: Julie Valenzuela, Nicholas Carter, Brandon Parker, Edward Lineen, Gabriel Ruiz 6/13/2024 Approval: Vilella, Namias
Purpose
- Identify patients appropriate for direct ortho trauma service admission.
- Standardize admission and transfer of patients to Ortho Trauma Service or to the Trauma Service.
- Streamline and harmonize the processes
- If the trauma attending surgeon considers a patient appropriate for admission to orthopedic service but the orthopedic resident has remaining concerns, the attending orthopedic surgeon should be contacted by the orthopedic resident to contact the attending trauma surgeon directly for further discussion.
Scope
- This guideline will apply to patients at Jackson Memorial and Ryder Trauma Center
Definition
- Isolated orthopedic injuries include those injuries confined to the extremities that consist primarily of bone and joint involvement. This includes both operative and non-operative pathologies.
- Soft tissue injury associated to fracture or isolated ligament/tendon/cartilage does not preclude orthopedic admission.
Exceptions
- 2 or more long bone fractures (femur, tibia, humerus, radial/ulnar shaft)
- Tibia/Fibula and Radius/Ulna considered as one
- Bilateral acetabulum fractures
- Patient’s meeting criteria for G65 (geriatric service)
- Involvement of another system requiring admission
- Pulmonary contusions as defined bt trauma attending
- Unilateral acetabulum fracture in geriatric population (>65)
- Pelvic injury
- Any long bone or pelvis injury requiring blood transfusion as part of initial resuscitation.
- Hemodynamically unstable (defined at attending level) after initial resuscitation or requiring blood transfusion for resuscitation.
- Presence of High Risk characteristics as defined in Section V
High-Risk definition or special considerations for Orthopedic admission exception
- Cardiac disease (MI within last 6 months, active myocardial ischemia, CHF)
- Pulmonary disease requiring home oxygen
- Significant Liver disease (MELD >20)
- ESRD on dialysis
- Home anticoagulation (excluding ASA)
- Pregnancy
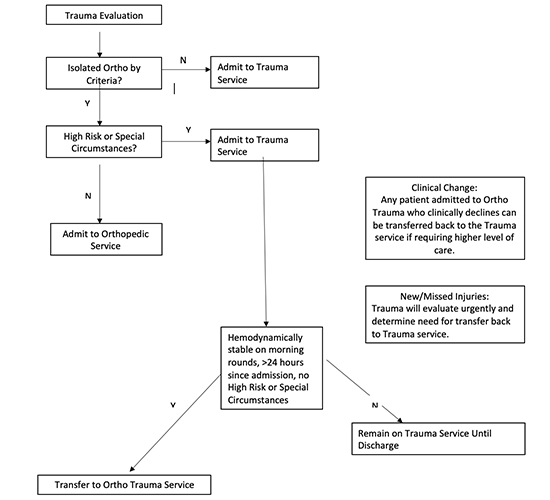
Process/Algorithm
- If patient has polytrauma or isolated ortho exclusions, Trauma will admit.
- If meets isolated ortho definition, assess for high risk comorbidities.
- If patient has at least one high risk comorbidity (as above), Trauma will admit.
- If patient does not have high risk comorbidity, admission to Orthopedic service.
Isolated ortho trauma with hemodynamic instability
- If the patient is hemodynamically unstable (requiring blood in the ED), the patient will be admitted to the Trauma service for 24 hours.
- If the patient has stabilized hemodynamically, normal (or normalizing) lactate and oxygen saturation greater than 95% on room air) at 24 hrs after admission, the patient will transfer to the Ortho Trauma service via the transfer pathway below.
- If the patient remains hemodynamically unstable 24 hours after admission, the patient will remain on the trauma service until discharge.
New or missed injuries:
- Trauma will evaluate urgently and determine need for transfer back to the Trauma service in discussion with Ortho Trauma team.
Clinical Change Pathway
- Any Ortho Trauma patient admitted to Ortho Trauma that experiences clinical change and requires transfer to higher level of care (ICU or stepdown unit), patient will be transferred back to the Trauma service.
Service Transfer
- Patients who meet criteria to be transferred from the Trauma Service to the Orthopedic Surgery service will occur after the required 24 hours of observation.
- This will occur between 6am and 6pm
Algorithm for Ortho Trauma Admissions for Patients Arriving to Trauma Resus via EMS
Purpose
- Identify patients appropriate for direct ortho trauma service admission.
- Standardize admission and transfer of patients to Ortho Trauma Service or to the Trauma Service.
- Streamline and harmonize the processes
- If the trauma attending surgeon considers a patient appropriate for admission to orthopedic service but the orthopedic resident has remaining concerns, the attending orthopedic surgeon should be contacted by the orthopedic resident to contact the attending trauma surgeon directly for further discussion.
Scope
- This guideline will apply to patients at Jackson Memorial and Ryder Trauma Center
Definition
- Isolated orthopedic injuries include those injuries confined to the extremities that consist primarily of bone and joint involvement. This includes both operative and non-operative pathologies.
- Soft tissue injury associated to fracture or isolated ligament/tendon/cartilage does not preclude orthopedic admission.
Exceptions
- 2 or more long bone fractures (femur, tibia, humerus, radial/ulnar shaft)
- Tibia/Fibula and Radius/Ulna considered as one
- Bilateral acetabulum fractures
- Patient’s meeting criteria for G65 (geriatric service)
- Involvement of another system requiring admission
- Pulmonary contusions as defined bt trauma attending
- Unilateral acetabulum fracture in geriatric population (>65)
- Pelvic injury
- Any long bone or pelvis injury requiring blood transfusion as part of initial resuscitation.
- Hemodynamically unstable (defined at attending level) after initial resuscitation or requiring blood transfusion for resuscitation.
- Presence of High Risk characteristics as defined in Section V
High-Risk definition or special considerations for Orthopedic admission exception
- Cardiac disease (MI within last 6 months, active myocardial ischemia, CHF)
- Pulmonary disease requiring home oxygen
- Significant Liver disease (MELD >20)
- ESRD on dialysis
- Home anticoagulation (excluding ASA)
- Pregnancy
Process/Algorithm
- If patient has polytrauma or isolated ortho exclusions, Trauma will admit.
- If meets isolated ortho definition, assess for high risk comorbidities.
- If patient has at least one high risk comorbidity (as above), Trauma will admit.
- If patient does not have high risk comorbidity, admission to Orthopedic service.
Isolated ortho trauma with hemodynamic instability
- If the patient is hemodynamically unstable (requiring blood in the ED), the patient will be admitted to the Trauma service for 24 hours.
- If the patient has stabilized hemodynamically, normal (or normalizing) lactate and oxygen saturation greater than 95% on room air) at 24 hrs after admission, the patient will transfer to the Ortho Trauma service via the transfer pathway below.
- If the patient remains hemodynamically unstable 24 hours after admission, the patient will remain on the trauma service until discharge.
New or missed injuries:
- Trauma will evaluate urgently and determine need for transfer back to the Trauma service in discussion with Ortho Trauma team.
Clinical Change Pathway
- Any Ortho Trauma patient admitted to Ortho Trauma that experiences clinical change and requires transfer to higher level of care (ICU or stepdown unit), patient will be transferred back to the Trauma service.
Service Transfer
- Patients who meet criteria to be transferred from the Trauma Service to the Orthopedic Surgery service will occur after the required 24 hours of observation.
- This will occur between 6am and 6pm
Algorithm for Ortho Trauma Admissions for Patients Arriving to Trauma Resus via EMS