Direct Peritoneal Resuscitation (DPR)
Authors: Matthew Fleming, Zenia Jenkins, Roberto Blanco, Jonathan Meizoso, Nicholas Carter
Date: July 2025
Approval: Nicholas Namias
Indications and Benefits:
- In patients suffering major abdominal trauma or emergency general surgery for peritonitis, direct peritoneal resuscitation (DPR) has been associated with the following benefits: net removal of fluid from edematous tissue, faster time to abdominal closure (2-3 days earlier), >90% likelihood of primary fascial closure, fewer intra-abdominal complications requiring percutaneous or open procedures, and fewer enterocutaneous fistulas.
- DPR should be considered in any patient requiring damage control laparotomy. For patients whose abdomen is not closed at the first reoperation, DPR should be strongly considered at each takeback until the abdomen is closed.
Indications and Benefits:
- In patients suffering major abdominal trauma or emergency general surgery for peritonitis, direct peritoneal resuscitation (DPR) has been associated with the following benefits: net removal of fluid from edematous tissue, faster time to abdominal closure (2-3 days earlier), >90% likelihood of primary fascial closure, fewer intra-abdominal complications requiring percutaneous or open procedures, and fewer enterocutaneous fistulas.
- DPR should be considered in any patient requiring damage control laparotomy. For patients whose abdomen is not closed at the first reoperation, DPR should be strongly considered at each takeback until the abdomen is closed.
You are just about to enter a carousel of images of 2 slides.
You are just about to enter a carousel of images of 2 slides.
Configuration:
- Standard open abdomen equipment: sterile silastic sheet with puncture holes, JP drains x2 directed laterally, Ioban with good seal. Avoid Abthera due to limited capacity of vac cannister.
- – Outflow via standard temporary closure Y-connector with cut pieces of suction tubing to JP drains
You are just about to enter a carousel of images of 2 slides.
You are just about to enter a carousel of images of 2 slides.
You are just about to enter a carousel of images of 2 slides.
Fluid inflow:
- 19 French round drain directed towards root of mesentery secured at LUQ (or wherever is convenient based on surgical approach)
- Inflow from pump with fluid warmer via needleless catheter adapter
You are just about to enter a carousel of images of 2 slides.
Support Groups
You are just about to enter a carousel of images of 2 slides.
Configuration:
- Standard open abdomen equipment: sterile silastic sheet with puncture holes, JP drains x2 directed laterally, Ioban with good seal. Avoid Abthera due to limited capacity of vac cannister.
- – Outflow via standard temporary closure Y-connector with cut pieces of suction tubing to JP drains
You are just about to enter a carousel of images of 2 slides.
You are just about to enter a carousel of images of 2 slides.
Fluid inflow:
- 19 French round drain directed towards root of mesentery secured at LUQ (or wherever is convenient based on surgical approach)
- Inflow from pump with fluid warmer via needleless catheter adapter
You are just about to enter a carousel of images of 2 slides.
What fluid to use:
- 2.5% glucose based peritoneal dialysis fluid
How much fluid to give:
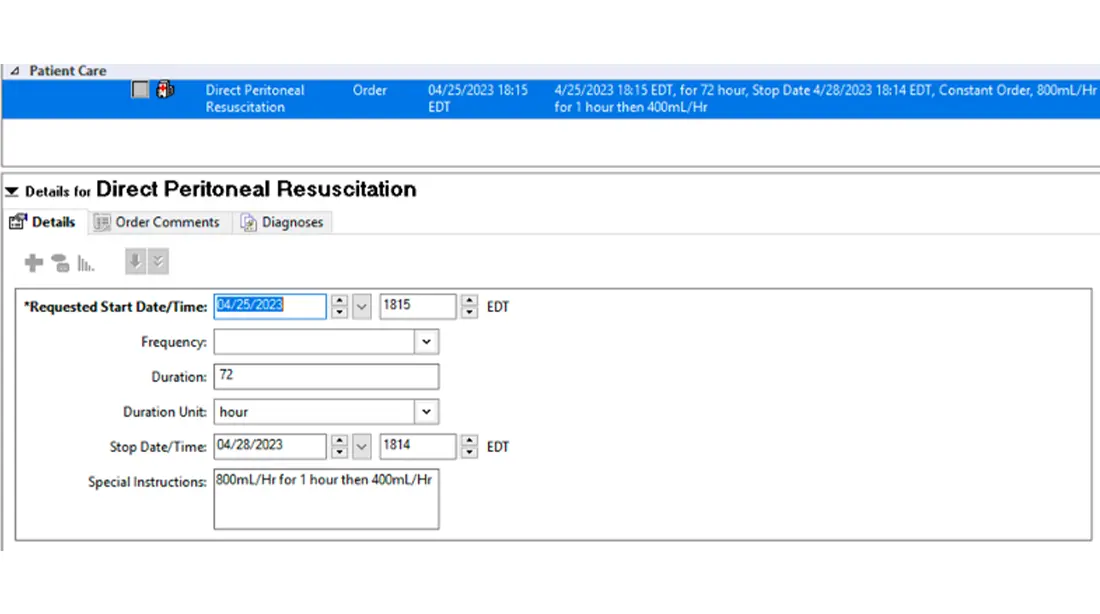
- Recommended starting rate is 800cc/hr for first hour
- Then decrease rate to 400cc/hr or 5cc/kg (if you can verify the weight of patient) for duration of DPR therapy
How to order in Cerner:
What fluid to use:
- 2.5% glucose based peritoneal dialysis fluid
How much fluid to give:
- Recommended starting rate is 800cc/hr for first hour
- Then decrease rate to 400cc/hr or 5cc/kg (if you can verify the weight of patient) for duration of DPR therapy
How to order in Cerner:
These guidelines were prepared by trauma division medical staff based on current review of medical literature and practice. They should be considered general practice guidelines and not protocols or policies. All management should be at the discretion of the responsible physician.
REFERENCES:
Kim, W.C., Tesoriero, R.B. & Stein, D.M. We Asked the Experts: Direct Peritoneal Resuscitation: A Modern Adaptation of a Historical Technique.World J Surg 44, 2982–2984 (2020). https://doi.org/10.1007/s00268-020-05569-0. PMID: 32409864.
Pera SJ, Schucht J, Smith JW. Direct Peritoneal Resuscitation for Trauma. Adv Surg. 2022 Sep;56(1):229-245. doi: 10.1016/j.yasu.2022.03.003. Epub 2022 Jul 20. PMID: 36096569.
Ribeiro-Junior MAF, Costa CTK, de Souza Augusto S, Néder PR, Elia YGB, Rattan R; Peritoneal Resuscitation Study Group; Di Saverio S. The role of direct peritoneal resuscitation in the treatment of hemorrhagic shock after trauma and in emergency acute care surgery: a systematic review. Eur J Trauma Emerg Surg. 2022 Apr;48(2):791-797. doi: 10.1007/s00068-021-01821-x. Epub 2021 Nov 13. PMID: 34773466.
Smith JW, Garrison RN, Matheson PJ et al. Direct peritoneal resuscitation accelerates primary abdominal wall closure after damage control surgery. J Am Coll Surg 2010(5):658–664. PMID: 20421025.
Smith JW, Garrison RN, Matheson PJ et al. Adjunctive treatment of abdominal catastrophes and sepsis with direct peritoneal resuscitation: Indications for use in acute care surgery. JTACS 2014 77(3): p393-399. PMID: 25159241.
Weaver JL, Smith JW. Direct Peritoneal Resuscitation: A Review. Int J Surg 2016(33): p237-241. PMID: 26384838.
Wiseman S, Harvey EM, Bower KL. Direct Peritoneal Resuscitation: A Novel Adjunct to Damage Control Laparotomy. Crit Care Nurse. 2019 Dec 1;39(6):37-45. doi: 10.4037/ccn2019397. PMID: 31961935.
Description
These guidelines were prepared by trauma division medical staff based on current review of medical literature and practice. They should be considered general practice guidelines and not protocols or policies. All management should be at the discretion of the responsible physician.
REFERENCES:
Kim, W.C., Tesoriero, R.B. & Stein, D.M. We Asked the Experts: Direct Peritoneal Resuscitation: A Modern Adaptation of a Historical Technique.World J Surg 44, 2982–2984 (2020). https://doi.org/10.1007/s00268-020-05569-0. PMID: 32409864.
Pera SJ, Schucht J, Smith JW. Direct Peritoneal Resuscitation for Trauma. Adv Surg. 2022 Sep;56(1):229-245. doi: 10.1016/j.yasu.2022.03.003. Epub 2022 Jul 20. PMID: 36096569.
Ribeiro-Junior MAF, Costa CTK, de Souza Augusto S, Néder PR, Elia YGB, Rattan R; Peritoneal Resuscitation Study Group; Di Saverio S. The role of direct peritoneal resuscitation in the treatment of hemorrhagic shock after trauma and in emergency acute care surgery: a systematic review. Eur J Trauma Emerg Surg. 2022 Apr;48(2):791-797. doi: 10.1007/s00068-021-01821-x. Epub 2021 Nov 13. PMID: 34773466.
Smith JW, Garrison RN, Matheson PJ et al. Direct peritoneal resuscitation accelerates primary abdominal wall closure after damage control surgery. J Am Coll Surg 2010(5):658–664. PMID: 20421025.
Smith JW, Garrison RN, Matheson PJ et al. Adjunctive treatment of abdominal catastrophes and sepsis with direct peritoneal resuscitation: Indications for use in acute care surgery. JTACS 2014 77(3): p393-399. PMID: 25159241.
Weaver JL, Smith JW. Direct Peritoneal Resuscitation: A Review. Int J Surg 2016(33): p237-241. PMID: 26384838.
Wiseman S, Harvey EM, Bower KL. Direct Peritoneal Resuscitation: A Novel Adjunct to Damage Control Laparotomy. Crit Care Nurse. 2019 Dec 1;39(6):37-45. doi: 10.4037/ccn2019397. PMID: 31961935.